Atlantoaxial Instability







Atlantoaxial Instability Definition
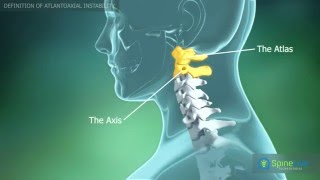
Atlantoaxial Instability is a condition that is characterized by an excess of movement between the vertebrae in the neck known as the atlas and the axis. Speaking of Atlantoaxial instability definition, this condition is considered as a result of an abnormality in the bones or the ligaments. If the nerve roots or the spinal cord are affected, neurologic symptoms can result as a complication of Atlantoaxial Instability.
Atlantoaxial Instability can be due to congenital conditions, but when the condition occurs in adults, it is usually due to degenerative changes related to Rheumatoid Arthritis or due to acute trauma. The infection has also been found to cause Atlantoaxial Instability. This is because the area has a rich supply of blood which provides a route for complications of infections to develop.
There are many congenital causes of Atlantoaxial Instability. These include:
-
- - Down Syndrome
-
- - Larsen Syndrome
-
- - Osteogenesis Imperfecta
-
- - Morquio Syndrome
-
- - Spondylotic-Epiphyseal Dysplasia (SED)
-
- - Neurofibromatosis
-
- - Meta tropic Dysplasia
-
- - Kniest Syndrome
-
- - Chondrodysplasia Punctata
Other diseases that can result in Atlantoaxial Instability include diseases that involve bone structure or metabolism or the characteristics of the ligaments.
Reasons
Atlantoaxial Instability can occur due to abnormalities in the bones or can be the result of abnormal development, or an ossification or fracture of the odontoid process (peg) of the axis, without or with remodelling.
It is not known what happens in the transverse ligament that leads to Atlantoaxial Instability. It could be that an abnormal protein in the connective tissue causes the lack of tension in the ligament that is seen in people with Down syndrome. Ligament inflammation that occurs in people with Rheumatoid Arthritis or infections who have Atlantoaxial Instability, can weaken the joint and this leads to subluxation (dislocation).
Conditions associated with atlantoaxial instability include:
-
- -Down Syndrome
- -Larsen Syndrome
- -Congenital Scoliosis
- -Neurofibromatosis
- -Osteogenesis Imperfecta
- -SED Congenita
- -Morquio Syndrome
- -Chondrodysplasia Punctata
- -Kniest Syndrome
- -Metatropic Dysplasia
- -Os Odontoideum
- -Odontoid Abnormalities
- -Third Condyle
- -Ossiculum Terminale
- -Hypoplasia or absence of the dens
- -Pseudoachondroplasia
- -Achondroplasia
- -Rheumatoid arthritis
- -Cartilage-hair hyperplasia
- -Ankylosing Spondylitis
- -Steroid therapy
- -Scott Syndrome
- -Trauma
- -Tumors
- -Cerebral Palsy
- -Infections of the head and neck
Prevalence
United States Statistics
Atlantoaxial Instability is extremely rare in people who do not have factors that predispose them to the development of the condition. There is no data in existence related to the prevalence of the condition when risk factors are absent. Among people who have Down Syndrome, Asymptomatic Atlantoaxial Instability occurs at a frequency of approximately 13% based on some studies. The symptomatic type of the condition was found to occur at a frequency of approximately 1.5% in Down Syndrome patients.
In people who have Rheumatoid Arthritis, the rate of Atlantoaxial Instability or AAS has been estimated at approximately 20%, but it occurs in up to 49% of older individuals who have RA according to some other research studies.
Other demographics
Atlantoaxial Instability does not appear strongly preponderant in any specific age group. Individuals more at risk are those younger people who have Down Syndrome and older people who have Rheumatoid Arthritis. Also, Grisel Syndrome occurs more frequently in children, however, AAS can develop after an infection of the nose and throat. Most of these conditions resolve without the patient ever being seen for medical treatment.
No association with gender has been observed with Idiopathic Atlantoaxial Instability, but other disorders that could lead to developing the condition may be more prevalent in one sex than the other. For instance, Rheumatoid Arthritis occurs in women nearly five times more often than it does in men.
There is no recognized racial predilection for Atlantoaxial Instability.
Complications
Prognosis is typically good for patients who have Symptomatic Atlantoaxial Instability when they have a posterior spinal fusion and their function returns. Surgery may be able to decrease symptoms of Myelopathy, relieve pain, or accomplish both in many people. Results and outcome are dependent on the cause of the instability and the severity of symptoms.
Extreme ranges of motion can make patients susceptible to an arising or even worsening spinal cord compression. There are symptoms of Neurologic Dysfunction progression such as:
-
- - Myelopathy
-
- - Spasticity
-
- - Radicular symptoms
-
- - Neck and shoulder pain
Mortality and Morbidity
For most people, pain is the most common symptom experienced by patients with Atlantoaxial Instability. Pain is typically either a headache or vague pain in the neck pain. Pain is typically nonspecific and many times, patients require further evaluation to determine the exact source. Due to the location of the spinal cord and the blood vessels to the vertebrae in this area, additional serious complications like Vascular Occlusion or Myelopathy are possible.
Neurologic signs and symptoms include loss of coordination, clumsiness, difficulty walking, abnormal gait, easy fatigue, limited neck mobility and pain, torticollis, neurogenic bladder, sensory deficits, upper motor neuron signs (Hyperreflexia, Spasticity, Babinski sign, Clonus), Hemiplegia, Paraplegia, and Quadriplegia. Any person who is at risk for Atlantoaxial Instability and develops these symptoms should be urgently evaluated.
You may also be interested in Piriformis Syndrome
Atlantoaxial Instability Treatment and Care
Non-Surgical Treatments
Non-surgical medications for Spinal Instability are normally enough to limit the side effects of Atlantoaxial Instability and the numerous wounds of the spine including patients with a back pain Non-steroidal calming solution along with non-intrusive treatment and endorsed practices regularly works well. Ergonomics are imperative to prevent setting the neck in an unstable place (regularly a flexing and twisting movement). Chiropractic control of Spinal Instability is not suggested as these portions move excessively and control would expand the movement.
Surgical Treatments for Spinal Instability
In the event that these non-surgical treatments don't work, and the patient is having progressing back pain and weakness, surgery for the neck including neck adjustments will no doubt be the following course of Spinal Instability treatment.
The Anterior Cervical Discectomy Fusion (ACDF) system is performed for Atlantoaxial Instability, degenerative disc disease, bone spurs, compressed nerves (neck), or spinal cord, herniated disc, or even a crack in the atlantoaxial spine.
Physical Therapy
The objective of the physical therapy is to upgrade the capacity of the spine by balancing out subsystems and diminishing the weights on the affected spinal fragments.
Posture and spinal control:
-
- - Decreases weights on the detached subsystem.
Proper stance:
-
- - Diminishes the heaps put on the spinal portions at end-ranges and returns the spine to a biomechanically effective position.
Spinal control can be accomplished on spinal fragments above and underneath the level of instability and will help with spinal movement over some of the sections. Additionally, the weights on the level of Atlantoaxial Instability are accepted to be decreased.
Strengthening helps:
-
- - Enhances the capacity of the dynamic subsystem.
-
- - The atlantoaxial multifidus may give steadiness via segmental connections to atlantoaxial vertebrae.
-
- - The m.longus colli and capitus give foremost strength.
Strengthening the muscles may empower those muscles to enhance the quality and control of development happening inside the impartial zone and help with spinal instability.
The patient with Spinal Instability is not required to wear a support. Following a month and a half, the patient is not urged to do any lifting more than 4kg. The restoration starts at week 6, mainly, a fundamental steadiness therapy program.
The utilization of stance instruction and spinal control might be utilized to diminish weight on the inactive subsystem. Spinal control can be performed on hypo mobile spinal portions above and underneath the precariousness level. It is trusted that with those controls the spinal development is all the more uniformly appropriated over the portions and that mechanical weight on clinical insecurity is diminished.
One of the fundamental objectives of the non-surgical of Atlantoaxial Instability treatment is to enhance the nature of the controlled movement. Subsequently, proprioception practices must be utilized, this will enhance the control of development in the unbiased zone. Another imperative objective is to diminish the weight of the cervical locale, utilizing delicate tissue methods. By accomplishing these objectives surgery might be counteracted.
Pathological Changes of Atlantoaxial Instability
Atlantoaxial Instability can occur due to trauma or due to abnormalities that are associated with the first two vertebrae of the cervical spine, where the joints come together. This causes excessive movement in the joint. There are typically three patterns noted in the movement of spinal instability:
-
- -Distraction
-
- -Rotation
-
- -Flexion-extension
Most commonly, abnormalities involve the odontoid process or the transverse ligament. The transverse ligament is very strong and it and the joint capsules help to maintain the connection between the atlas and the axis, the first two cervical vertebrae.
In people with Down Syndrome, the main cause of Atlantoaxial Instability is the loss of tension in the transverse ligament. Other conditions that are present at birth can be associated with spinal instability. These include:
-
- -Osteogenesis Imperfecta
-
- -Congenital Scoliosis
-
- -Neurofibromatosis
-
- -Larsen Syndrome
-
- -Morquio Syndrome
-
- -SED Congenita
-
- -Metatropic Dysplasia
-
- -Chondrodysplasia Punctata
-
- -Kniest Syndrome
Odontoid anomalies can also cause Atlantoaxial Instability. These include Os Terminale, Aplasia, Duplication, Hypoplasia, Third Condyle, and Os Odontoideum. Atlanto-occipital fusion can also make it more likely that a person will develop Atlantoaxial Instability.

Atlantoaxial Instability Symptoms
Atlantoaxial Instability symptoms may not even show up. A few patients encounter aching, for example, an "undetermined neck pain or a headache". Since the vascular supply and spinal cord are adjacent to each other, vascular myelopathy could probably happen.
There are neurological manifestations as well. Patients may have problems with coordination, and experience abnormal steps, awkwardness, have trouble walking, restricted portability, torticollis, and they may turn out to be effortlessly exhausted.
Atlantoaxial Instability Symptoms
Atlantoaxial Instability symptoms may not even show up. A few patients encounter aching, for example, an "undetermined neck pain or a headache". Since the vascular supply and spinal cord are adjacent to each other, vascular myelopathy could probably happen.
There are neurological manifestations as well. Patients may have problems with coordination, and experience abnormal steps, awkwardness, have trouble walking, restricted portability, torticollis, and they may turn out to be effortlessly exhausted. It is also possible that "Paraplegia, Hemiplegia, and Quadriplegia" could happen.
Patients with hazardous Atlantoaxial Instability symptoms need to be seen by a medical professional who's proficient in "radiographic and surgical assessments". Atlantoaxial Instability symptoms can progress, which can cause spinal cord compression and complexities of Myelopathy and neck pain, as well as spasticity and radicular symptoms too.
Atlantoaxial Instability symptoms inside the lower spine include lower back pain with an on-going sensation inside the area. Numerous patients think that it's hard to twist their midsection. Muscle fits are additionally a typical event for patients encountering instability. A painful back can happen with movement and an ill-equipped patient may suffer more than necessary.
Common Symptoms
The most common Atlantoaxial Instability symptom is an excess in the movement of the cervical region of the spine. Neck pain due to Atlantoaxial Instability occurs when the spinal cord or its nerves are affected. Usually, neck pain due to Atlantoaxial Instability increases with movement and is relieved by rest. If Atlantoaxial Instability causes the compression of nerve roots, Atlantoaxial Instability symptoms such as occipital headaches may occur.
Compression of the spinal cord due to Atlantoaxial Instability produces weakness, spasticity, tingling, and changes in sensation in the lower and upper extremities.
In extremely rare cases, when Atlantoaxial Instability symptoms cause compression of the spinal cord, a person's bladder and bowel function may be disrupted.
Here's a list of atlantoaxial instability symptoms:
-
- -Chronic pain
-
- -Headaches
-
- -Limited range of neck movement
-
- -Spinal cord compression
-
- -Torticollis
-
- -Muscular weakness
-
- -Spasticity
-
- -Walking problems
Diagnostic Procedures
The determination of lumbar weakness is normally found in light of the imaging finding of irregular vertebral movement.
Atlantoaxial Instability symptoms can be diagnosed by a patient's medical history and physical examination on the grounds that there is yet to be standardized X-rays or imaging that's ready to analyze Atlantoaxial Instability or distinguish a cracked ligamentous tissue without the presence of an injury.
Moreover, there is little relationship between the level of instability or hypermobility that appeared on radiographic studies and clinical symptoms. Even after extreme whiplash wounds, plain radiographs are normal in spite of clinical discoveries demonstrating the presence of the tissue damage.
-
- X-rays could be helpful to screen the uprightness of the vertebral tendons. Taking pictures during a shear test or a diversion test demonstrates a more noteworthy intervertebral separation and an expansion in coordinate length of the tendons.
-
- Functional Computerized Tomography (FCT) and Magnetic Resonance Imaging (fMRI) can also help determine Atlantoaxial Instability pathology. Studies utilizing FCT for diagnosing delicate tissue ligament or post-whiplash wounds have exhibited the capacity of this procedure to indicate excess atlantooccipital and atlantoaxial movement during a rotation. This is particularly applicable when patients have signs and symptoms of Atlantoaxial Instability, yet have ordinary MRIs in an impartial position.
Rather than static standard films, functional imaging technology is needed for sufficient radiologic images of Atlantoaxial Instability. This is because they provide images of the neck when moving that are dynamic and are useful for the evaluation of the degree and presence of Atlantoaxial Instability.
"Paraplegia, Hemiplegia, and Quadriplegia" could happen.
Patients with hazardous Atlantoaxial Instability symptoms need to be seen by a medical professional who's proficient in "radiographic and surgical assessments". Atlantoaxial Instability symptoms can progress, which can cause spinal cord compression and complexities of Myelopathy and neck pain, as well as spasticity and radicular symptoms too.
Atlantoaxial Instability symptoms inside the lower spine include lower back pain with an on-going sensation inside the area. Numerous patients think that it's hard to twist their midsection. Muscle fits are additionally a typical event for patients encountering instability. A painful back can happen with movement and an ill-equipped patient may suffer more than necessary.
Common Symptoms
The most common Atlantoaxial Instability symptom is an excess in the movement of the cervical region of the spine. Neck pain due to Atlantoaxial Instability occurs when the spinal cord or its nerves are affected. Usually, neck pain due to Atlantoaxial Instability increases with movement and is relieved by rest. If Atlantoaxial Instability causes the compression of nerve roots, Atlantoaxial Instability symptoms such as occipital headaches may occur. Compression of the spinal cord due to Atlantoaxial Instability produces weakness, spasticity, tingling, and changes in sensation in the lower and upper extremities.
In extremely rare cases, when Atlantoaxial Instability symptoms cause compression of the spinal cord, a person's bladder and bowel function may be disrupted.
Here's a list of atlantoaxial instability symptoms:
-
- -Chronic pain
-
- -Headaches
-
- -Limited range of neck movement
-
- -Spinal cord compression
-
- -Torticollis
-
- -Muscular weakness
-
- -Spasticity
-
- -Walking problems
Diagnostic Procedures
The determination of lumbar weakness is normally found in light of the imaging finding of irregular vertebral movement. Atlantoaxial Instability symptoms can be diagnosed by a patient's medical history and physical examination on the grounds that there is yet to be standardized X-rays or imaging that's ready to analyze Atlantoaxial Instability or distinguish a cracked ligamentous tissue without the presence of an injury.
Moreover, there is little relationship between the level of instability or hypermobility that appeared on radiographic studies and clinical symptoms. Even after extreme whiplash wounds, plain radiographs are normal in spite of clinical discoveries demonstrating the presence of the tissue damage.
-
- X-rays could be helpful to screen the uprightness of the vertebral tendons. Taking pictures during a shear test or a diversion test demonstrates a more noteworthy intervertebral separation and an expansion in coordinate length of the tendons.
-
- Functional Computerized Tomography (FCT) and Magnetic Resonance Imaging (fMRI) can also help determine Atlantoaxial Instability pathology. Studies utilizing FCT for diagnosing delicate tissue ligament or post-whiplash wounds have exhibited the capacity of this procedure to indicate excess atlantooccipital and atlantoaxial movement during a rotation. This is particularly applicable when patients have signs and symptoms of Atlantoaxial Instability, yet have ordinary MRIs in an impartial position.
Rather than static standard films, functional imaging technology is needed for sufficient radiologic images of Atlantoaxial Instability. This is because they provide images of the neck when moving that are dynamic and are useful for the evaluation of the degree and presence of Atlantoaxial Instability.

 Spine
Spine